The Cause Of Bursitis Of The Feet?
Overview
Infracalcaneal bursitis (inflammation of the bursa below the calcaneus, or heel bone) is one of the most common types of bursitis in the foot. Infracalcaneal bursitis can sometimes be difficult to differentiate from plantar fasciosis-another condition that causes pain below the heel. The key difference is that infracalcaneal bursitis tends to be worse at the end of the day whereas plantar fascia pain tends to be worse in the morning, immediately upon waking.
Causes
Bursitis occurs when the synovial lining becomes thickened and produces excessive fluid, leading to localized swelling and pain. It most commonly affects the subacromial, olecranon, trochanteric, prepatellar, and infrapatellar bursae. Symptoms of bursitis may include localized tenderness, pain, edema, erythema, or reduced movement. Pain is aggravated by movement of the specific joint, tendon, or both.
Symptoms
Symptoms of bursitis include pain in the heel, especially with walking, running, or when the area is touched. The skin over the back of the heel may be red and warm, and the pain may be worse with attempted toe rise (standing on tippy-toes).
Diagnosis
The doctor will discuss your symptoms and visually assess the bones and soft tissue in your foot. If a soft tissue injury is suspected, an MRI will likely be done to view where and how much the damage is in your ankle. An x-ray may be recommended to rule out a bone spur or other foreign body as the cause of your ankle pain. As the subcutaneous bursa is close to the surface of the skin, it is more susceptible to septic, or infectious, bursitis caused by a cut or scrape at the back of the heel. Septic bursitis required antibiotics to get rid of the infection. Your doctor will be able to determine whether there is an infection or not by drawing a small sample of the bursa fluid with a needle.
Non Surgical Treatment
Treatment for soft tissue conditions focuses on reducing pain and inflammation, and on preserving mobility and preventing disability and recurrence. The treatment for many soft tissue conditions is similar. A doctor's recommendations may include a combination of rest, splints, heat and cold application, medications, physical therapy, or occupational therapy. A person with a soft tissue condition may try several treatments before he or she finds the best one for his or her specific condition.
Surgical Treatment
Surgery is rarely need to treat most of these conditions. A patient with a soft tissue rheumatic syndrome may need surgery, however, if problems persist and other treatment methods do not help symptoms.
Infracalcaneal bursitis (inflammation of the bursa below the calcaneus, or heel bone) is one of the most common types of bursitis in the foot. Infracalcaneal bursitis can sometimes be difficult to differentiate from plantar fasciosis-another condition that causes pain below the heel. The key difference is that infracalcaneal bursitis tends to be worse at the end of the day whereas plantar fascia pain tends to be worse in the morning, immediately upon waking.
Causes
Bursitis occurs when the synovial lining becomes thickened and produces excessive fluid, leading to localized swelling and pain. It most commonly affects the subacromial, olecranon, trochanteric, prepatellar, and infrapatellar bursae. Symptoms of bursitis may include localized tenderness, pain, edema, erythema, or reduced movement. Pain is aggravated by movement of the specific joint, tendon, or both.
Symptoms
Symptoms of bursitis include pain in the heel, especially with walking, running, or when the area is touched. The skin over the back of the heel may be red and warm, and the pain may be worse with attempted toe rise (standing on tippy-toes).
Diagnosis
The doctor will discuss your symptoms and visually assess the bones and soft tissue in your foot. If a soft tissue injury is suspected, an MRI will likely be done to view where and how much the damage is in your ankle. An x-ray may be recommended to rule out a bone spur or other foreign body as the cause of your ankle pain. As the subcutaneous bursa is close to the surface of the skin, it is more susceptible to septic, or infectious, bursitis caused by a cut or scrape at the back of the heel. Septic bursitis required antibiotics to get rid of the infection. Your doctor will be able to determine whether there is an infection or not by drawing a small sample of the bursa fluid with a needle.
Non Surgical Treatment
Treatment for soft tissue conditions focuses on reducing pain and inflammation, and on preserving mobility and preventing disability and recurrence. The treatment for many soft tissue conditions is similar. A doctor's recommendations may include a combination of rest, splints, heat and cold application, medications, physical therapy, or occupational therapy. A person with a soft tissue condition may try several treatments before he or she finds the best one for his or her specific condition.
Surgical Treatment
Surgery is rarely need to treat most of these conditions. A patient with a soft tissue rheumatic syndrome may need surgery, however, if problems persist and other treatment methods do not help symptoms.
Hammertoes Treatment
 Overview
Overview
Hammer toes most commonly affects the second toe on the foot. It causes the middle joint to bend. Hammertoe is most frequently caused by structural problems in the toe or from wearing poor fitting shoes. It is important to diagnose and treat hammertoe early because the condition tends to become worse over time. If left untreated, hammertoe can require surgery.
Causes
While there are a number of causes, there aren't many specific risk factors for hammertoes, women tend to get these problems more than men, but they occur without rhyme or reason. Diabetics, however, are more likely to get a hammertoe if they have underlying nerve damage in the toes and feet.
 Symptoms
Symptoms
Hammer toe is often distinguished by a toe stuck in an upside-down ?V? position, and common symptoms include corns on the top of your toe joint. Pain at the top of a bent toe when you put on your shoes. Pain when moving a toe joint. Pain on the ball of your foot under the bent toe. Corns developing on the top of the toe joint. It is advisable to seek medical advice if your feet hurt on a regular basis. It is imperative to act fast and seek the care of a podiatrist or foot surgeon. By acting quickly, you can prevent your problem from getting worse.
Diagnosis
Although hammertoes are readily apparent, to arrive at a diagnosis the foot and ankle surgeon will obtain a thorough history of your symptoms and examine your foot. During the physical examination, the doctor may attempt to reproduce your symptoms by manipulating your foot and will study the contractures of the toes. In addition, the foot and ankle surgeon may take x-rays to determine the degree of the deformities and assess any changes that may have occurred.
Non Surgical Treatment
A number of approaches can be undertaken to the manage a hammer toe. It is important that any footwear advice is followed. The correct amount of space in the toe box will allow room for the toes to function without excessive pressure. If a corn is present, this will need to be treated. If the toe is still flexible, it may be possible to use splints or tape to try and correct the toe. Without correct fitting footwear, this is often unsuccessful. Padding is often used to get pressure off the toe to help the symptoms. If conservative treatment is unsuccessful at helping the symptoms, surgery is often a good option.
Surgical Treatment
Surgery to correct for a hammertoe may be performed as a day procedure. There are several different types of procedures that can be used depending on the foot structure and if the deformity is flexible or rigid.
 Prevention
Prevention
wear sensible shoes. Here are some tips. Most people have one foot that's bigger than the other. Fit your shoes to the bigger foot. Buy your shoes at the end of the day as your feet tend to swell a bit and you will get a better sense of fit. When you buy your shoes, wear the sock that you will be using when wearing that shoe - wear a sports sock when buyingtrainers, for example. As you get older, your feet get bigger. Get your feet measured hammertoes every time you buy shoes. Don't go by shoe sizes. Shoe sizes vary among manufacturers; a shoe is the right size only when it fits comfortably. The ball of your foot should fit into the widest part of the shoe. A shoe should be sturdy so that it only bends in the ball of the foot, exactly where your big toes bend. Any shoe that can be bent anywhere along the sole or twisted side to side is generally too flimsy. There should be at least 1.5 cm between the tip of your longest toe and the front of the shoe. Never buy shoes that feel tight and expect them to stretch with wearing. If you have prominent areas on your feet such as hammer toes and bunions, avoid shoes with a lot of stitching or multiple pieces of fabric, as these stitched areas tend not to stretch to accommodate various toe deformities. Your shoes shouldn't ride up and down on your heel as you walk. The higher the heel, the less safe the shoe. Check children's shoes regularly.
What Are Hallux Valgus?
Overview
 A bunion is the enlargement of the joint at the base of the big toe. It occurs as a result of the misalignment of the bones of the big toe. This leads to stretching of the ligaments and tendons around the big toe joint and causes soft tissue over the joint to become inflamed and painful. There may be additional bone formation (exostosis) in the joint and the skin around the joint may become red and tender. Over time the cartilage in the joint can break down, leading to arthritis.
A bunion is the enlargement of the joint at the base of the big toe. It occurs as a result of the misalignment of the bones of the big toe. This leads to stretching of the ligaments and tendons around the big toe joint and causes soft tissue over the joint to become inflamed and painful. There may be additional bone formation (exostosis) in the joint and the skin around the joint may become red and tender. Over time the cartilage in the joint can break down, leading to arthritis.
Causes
Bunions are most often caused by faulty mechanics of the foot. The deformity runs in families, but it is the foot type that is hereditary, not the bunion.Certain foot types make a person prone to developing a bunion. Injury can be a cause, especially if just one foot is involved. Although wearing shoes that crowd the toes won?t actually cause bunions in the first place, it can make the deformity progressively worse. That means you may expererince symptoms sooner.
Symptoms
The symptoms of a bunion include the following development of a firm bump on the outside edge of the foot, at the base of the big toe, redness, swelling, or pain at or near the MTP joint, corns or other irritations caused by the overlap of the first and second toes, restricted or painful motion of the big toe.
Diagnosis
Clinical findings are usually specific. Acute circumferential intense pain, warmth, swelling, and redness suggest gouty arthritis (see Gout) or infectious arthritis (see Acute Infectious Arthritis), sometimes mandating examination of synovial fluid. If multiple joints are affected, gout or another systemic rheumatic disease should be considered. If clinical diagnosis of osteoarthritic synovitis is equivocal, x-rays are taken. Suggestive findings include joint space narrowing and bony spurs extending from the metatarsal head or sometimes from the base of the proximal phalanx. Periarticular erosions (Martel sign) seen on imaging studies suggest gout.
Non Surgical Treatment
Bunions can develop at any time. Although bunions often require no medical treatment you should consult your family doctor/chiropodist/podiatrist. Treatment options vary depending on the severity of your bunion and the amount of pain it causes you. Although they don't always cause problems, bunions are permanent unless surgically corrected. If the cushioning sac of fluid (bursa) over the affected joint becomes inflamed (bursitis), a bunion can be very painful and interfere with your normal activities. Bunions may get larger and more painful, making nonsurgical treatment less effective. Apply a non-medicated bunion pad around the bony bump. If a bunion becomes inflamed or painful, apply an ice pack two to three times daily to help reduce swelling. Wear shoes with a wide and deep toe box. Avoid shoes with heels higher than 2 inches (5.1 centimeters). 
Surgical Treatment
There is more than one way to surgically treat a bunion. While there are some general guidelines, some procedures work well for some Surgeons and poorly for others. Your Surgeon should consider the severity of your bunion, medical condition, lifestyle, and recuperation time when considering the surgical treatment.
What Causes Over-Pronation
Overview
Over-pronation, or flat feet, is a common biomechanical problem that occurs in the walking process when a person?s arch collapses upon weight bearing. This motion can cause extreme stress or inflammation on the plantar fascia, possibly causing severe discomfort and leading to other foot problems.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding stress to other parts of the foot. As a result, over-pronation, often leads to Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
Overpronation can be a contributing factor in other lower extremity disorders, such as foot pain, plantar fasciitis, ankle injuries, medial tibial stress syndrome (shin splints), periostitis, stress fractures and myofascial trigger points. Overpronation increases the degree of internal tibial rotation, thereby contributing to various knee disorders such as meniscal injury or ligament sprains. The effects of the postural deviation are exaggerated in athletes due to the increase in foot strikes while running and the greater impact load experienced. When running, three to four times the body weight is experienced with each foot strike.2 If overpronation exists, the shock force is not adequately absorbed by the foot and is transmitted further up the kinetic chain.
Diagnosis
People who overpronate have flat feet or collapsed arches. You can tell whether you overpronate by wetting your feet and standing on a dry, flat surface. If your footprint looks complete, you probably overpronate. Another way to determine whether you have this condition is to simply look at your feet when you stand. If there is no arch on the innermost part of your sole, and it touches the floor, you likely overpronate. The only way to truly know for sure, however, is to be properly diagnosed by a foot and ankle specialist.
Non Surgical Treatment
Overpronation is a condition in which the foot rolls excessively down and inward. The arch may elongate and collapse (or ?fall?) and the heel will lean inward. Overpronation should not be confused with pronation. Pronation is a normal motion of the foot during weight bearing and allows the foot to absorb shock as it contacts the ground.
Surgical Treatment
Depending on the severity of your condition, your surgeon may recommend one or more treatment options. Ultimately, however, it's YOUR decision as to which makes the most sense to you. There are many resources available online and elsewhere for you to research the various options and make an informed decision.
Over-pronation, or flat feet, is a common biomechanical problem that occurs in the walking process when a person?s arch collapses upon weight bearing. This motion can cause extreme stress or inflammation on the plantar fascia, possibly causing severe discomfort and leading to other foot problems.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding stress to other parts of the foot. As a result, over-pronation, often leads to Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
Overpronation can be a contributing factor in other lower extremity disorders, such as foot pain, plantar fasciitis, ankle injuries, medial tibial stress syndrome (shin splints), periostitis, stress fractures and myofascial trigger points. Overpronation increases the degree of internal tibial rotation, thereby contributing to various knee disorders such as meniscal injury or ligament sprains. The effects of the postural deviation are exaggerated in athletes due to the increase in foot strikes while running and the greater impact load experienced. When running, three to four times the body weight is experienced with each foot strike.2 If overpronation exists, the shock force is not adequately absorbed by the foot and is transmitted further up the kinetic chain.
Diagnosis
People who overpronate have flat feet or collapsed arches. You can tell whether you overpronate by wetting your feet and standing on a dry, flat surface. If your footprint looks complete, you probably overpronate. Another way to determine whether you have this condition is to simply look at your feet when you stand. If there is no arch on the innermost part of your sole, and it touches the floor, you likely overpronate. The only way to truly know for sure, however, is to be properly diagnosed by a foot and ankle specialist.
Non Surgical Treatment
Overpronation is a condition in which the foot rolls excessively down and inward. The arch may elongate and collapse (or ?fall?) and the heel will lean inward. Overpronation should not be confused with pronation. Pronation is a normal motion of the foot during weight bearing and allows the foot to absorb shock as it contacts the ground.
Surgical Treatment
Depending on the severity of your condition, your surgeon may recommend one or more treatment options. Ultimately, however, it's YOUR decision as to which makes the most sense to you. There are many resources available online and elsewhere for you to research the various options and make an informed decision.
How To Diagnose Calcaneal Apophysitis?
Overview
Sever's Disease is one of the most common causes of heel pain in active adolescents. Hip stability is restored using a non-surgical positioning device. Symptoms of Sever's disease are relieved through a combination of conservative treatment options and preventative measures can be taken to decrease the risk of developing the condition.
Causes
The calcaneal apophysis develops as an independent center of ossification (possibly multiple). It appears in boys aged 9-10 years and fuses by age 17 years, it appears in girls at slightly younger ages. During the rapid growth surrounding puberty, the apophyseal line appears to be weakened further because of increased fragile calcified cartilage. Microfractures are believed to occur because of shear stress leading to the normal progression of fracture healing. This theory explains the clinical picture and the radiographic appearance of resorption, fragmentation, and increased sclerosis leading to eventual union. The radiographs showing fragmentation of the apophysis are not diagnostic, because multiple centers of ossification may exist in the normal apophysis, as noted. However, the degree of involvement in children displaying the clinical symptoms of Sever disease appears to be more pronounced. In a study of 56 male students from a soccer academy, of whom 28 had Sever disease and 28 were healthy control subjects, findings suggested that higher heel plantar pressures under dynamic and static conditions were associated with Sever disease, though it was not established whether the elevated pressures predisposed to or resulted from the disease. Gastrocnemius ankle equinus also appeared to be a predisposing factor.
Symptoms
Symptoms of Sever?s disease, mostly pain at the back of heel, usually occur during and after sporting activity, and usually disappear with rest. In some cases, children may find it difficult to place pressure on their heels, and begin walking on their toes to gain relief. For some children, the heel pain will persist until the next morning, causing some stiffness or hobbling on first arising. Some children may experience mild swelling at the back of the heel.
Diagnosis
Physical examination varies depending on the severity and length of involvement. Bilateral involvement is present in approximately 60% of cases. Most patients experience pain with deep palpation at the Achilles insertion and pain when performing active toe raises. Forced dorsiflexion of the ankle also proves uncomfortable and is relieved with passive equinus positioning. Swelling may be present but usually is mild. In long-standing cases, the child may have calcaneal enlargement.
Non Surgical Treatment
Treatment of Severs disease usually involves a combination of an accurate analysis of your child?s gait, muscles, tendons, ligaments and joints is a crucial first step. Specific stretching and strengthening exercises often make up part of the treatment. Anti-inflammatory measures such as ice baths after exercise can be helpful in the short term. Footwear review, assessment and advice is important. Orthotic devices are often needed to firstly control any abnormal traction or tension on the heel growth plate and, secondly, too unload the ground reaction forces on the heel bone. Podiatry Care has podiatrists with specific paediatric training enabling them to utilise treatment options to relieve heel pain in children very quickly. If your child is struggling to play sport, see a Podiatry Care podiatrist near you. In severe cases modification to activity levels may be required. Treatment of Severs disease does NOT require surgery. This foot condition responds very well to conservative treatment.
Prevention
It is important to undertake correct warm ups and warm downs before and after exercise. This should include a stretching routine. It may be necessary to undertake additional stretching outside of sport, especially during stages of growth. Only playing one sport should be avoided. You should not allow your child to play through pain.
Sever's Disease is one of the most common causes of heel pain in active adolescents. Hip stability is restored using a non-surgical positioning device. Symptoms of Sever's disease are relieved through a combination of conservative treatment options and preventative measures can be taken to decrease the risk of developing the condition.
Causes
The calcaneal apophysis develops as an independent center of ossification (possibly multiple). It appears in boys aged 9-10 years and fuses by age 17 years, it appears in girls at slightly younger ages. During the rapid growth surrounding puberty, the apophyseal line appears to be weakened further because of increased fragile calcified cartilage. Microfractures are believed to occur because of shear stress leading to the normal progression of fracture healing. This theory explains the clinical picture and the radiographic appearance of resorption, fragmentation, and increased sclerosis leading to eventual union. The radiographs showing fragmentation of the apophysis are not diagnostic, because multiple centers of ossification may exist in the normal apophysis, as noted. However, the degree of involvement in children displaying the clinical symptoms of Sever disease appears to be more pronounced. In a study of 56 male students from a soccer academy, of whom 28 had Sever disease and 28 were healthy control subjects, findings suggested that higher heel plantar pressures under dynamic and static conditions were associated with Sever disease, though it was not established whether the elevated pressures predisposed to or resulted from the disease. Gastrocnemius ankle equinus also appeared to be a predisposing factor.
Symptoms
Symptoms of Sever?s disease, mostly pain at the back of heel, usually occur during and after sporting activity, and usually disappear with rest. In some cases, children may find it difficult to place pressure on their heels, and begin walking on their toes to gain relief. For some children, the heel pain will persist until the next morning, causing some stiffness or hobbling on first arising. Some children may experience mild swelling at the back of the heel.
Diagnosis
Physical examination varies depending on the severity and length of involvement. Bilateral involvement is present in approximately 60% of cases. Most patients experience pain with deep palpation at the Achilles insertion and pain when performing active toe raises. Forced dorsiflexion of the ankle also proves uncomfortable and is relieved with passive equinus positioning. Swelling may be present but usually is mild. In long-standing cases, the child may have calcaneal enlargement.
Non Surgical Treatment
Treatment of Severs disease usually involves a combination of an accurate analysis of your child?s gait, muscles, tendons, ligaments and joints is a crucial first step. Specific stretching and strengthening exercises often make up part of the treatment. Anti-inflammatory measures such as ice baths after exercise can be helpful in the short term. Footwear review, assessment and advice is important. Orthotic devices are often needed to firstly control any abnormal traction or tension on the heel growth plate and, secondly, too unload the ground reaction forces on the heel bone. Podiatry Care has podiatrists with specific paediatric training enabling them to utilise treatment options to relieve heel pain in children very quickly. If your child is struggling to play sport, see a Podiatry Care podiatrist near you. In severe cases modification to activity levels may be required. Treatment of Severs disease does NOT require surgery. This foot condition responds very well to conservative treatment.
Prevention
It is important to undertake correct warm ups and warm downs before and after exercise. This should include a stretching routine. It may be necessary to undertake additional stretching outside of sport, especially during stages of growth. Only playing one sport should be avoided. You should not allow your child to play through pain.
Tibial Posterior Tendon Dysfunction Stages
Overview
The majority of people will experience a flattening of the arch of the feet as we age. This is a natural part of the aging process for most, as the years of abuse we put on our feet causes weakening of the soft tissue structures that support the arch of the foot and gravity dictates that the feet tend to flatten out. When flattening of one of the feet occurs rapidly over a relatively short period of time this may signal a more serious problem. 
Causes
Flat footedness, most people who develop the condition already have flat feet. With overuse or continuous loading, a change occurs where the arch begins to flatten more than before, with pain and swelling developing on the inside of the ankle. Inadequate support from footwear may occasionally be a contributing factor. Trauma or injury, occasionally this condition may be due to fracture, sprain or direct blow to the tendon. Age, the risk of developing Posterior Tibial Tendon Dysfunction increases with age and research has suggested that middle aged women are more commonly affected. Other possible contributing factors - being overweight and inflammatory arthritis.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
Diagnostic testing is often used to diagnose the condition and help determine the stage of the disease. The most common test done in the office setting are weightbearing X-rays of the foot and ankle. These assess joint alignment and osteoarthritis. If tendon tearing or rupture is suspected, the gold standard test would be MRI. The MRI is used to check the tendon, surrounding ligament structures and the midfoot and hindfoot joints. An MRI is essential if surgery is being considered.
Non surgical Treatment
A patient who has acute tenosynovitis has pain and swelling along the medial aspect of the ankle. The patient is able to perform a single-limb heel-rise test but has pain when doing so. Inversion of the foot against resistance is painful but still strong. The patient should be managed with rest, the administration of appropriate anti-inflammatory medication, and immobilization. The injection of corticosteroids is not recommended. Immobilization with either a rigid below-the-knee cast or a removable cast or boot may be used to prevent overuse and subsequent rupture of the tendon. A removable stirrup-brace is not initially sufficient as it does not limit motion in the sagittal plane, a component of the pathological process. The patient should be permitted to walk while wearing the cast or boot during the six to eight-week period of immobilization. At the end of that time, a decision must be made regarding the need for additional treatment. If there has been marked improvement, the patient may begin wearing a stiff-soled shoe with a medial heel-and-sole wedge to invert the hindfoot. If there has been only mild or moderate improvement, a longer period in the cast or boot may be tried. 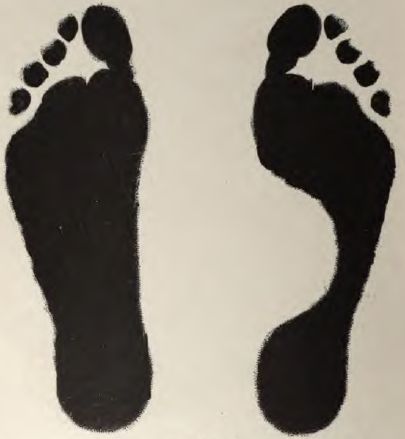
Surgical Treatment
In cases where cast immobilization, orthoses and shoe therapy have failed, surgery is the next alternative. The goal of surgery and non-surgical treatment is to eliminate pain, stop progression of the deformity and improve mobility of the patient. Opinions vary as to the best surgical treatment for adult acquired flatfoot. Procedures commonly used to correct the condition include tendon debridement, tendon transfers, osteotomies (cutting and repositioning of bone) and joint fusions. (See surgical correction of adult acquired flatfoot). Patients with adult acquired flatfoot are advised to discuss thoroughly the benefits vs. risks of all surgical options. Most procedures have long-term recovery mandating that the correct procedure be utilized to give the best long-term benefit. Most flatfoot surgical procedures require six to twelve weeks of cast immobilization. Joint fusion procedures require eight weeks of non-weightbearing on the operated foot - meaning you will be on crutches for two months. The bottom line is, Make sure all of your non-surgical options have been covered before considering surgery. Your primary goals with any treatment are to eliminate pain and improve mobility. In many cases, with the properly designed foot orthosis or ankle brace, these goals can be achieved without surgical intervention.