What Causes Over-Pronation
Overview
Over-pronation, or flat feet, is a common biomechanical problem that occurs in the walking process when a person?s arch collapses upon weight bearing. This motion can cause extreme stress or inflammation on the plantar fascia, possibly causing severe discomfort and leading to other foot problems.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding stress to other parts of the foot. As a result, over-pronation, often leads to Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
Overpronation can be a contributing factor in other lower extremity disorders, such as foot pain, plantar fasciitis, ankle injuries, medial tibial stress syndrome (shin splints), periostitis, stress fractures and myofascial trigger points. Overpronation increases the degree of internal tibial rotation, thereby contributing to various knee disorders such as meniscal injury or ligament sprains. The effects of the postural deviation are exaggerated in athletes due to the increase in foot strikes while running and the greater impact load experienced. When running, three to four times the body weight is experienced with each foot strike.2 If overpronation exists, the shock force is not adequately absorbed by the foot and is transmitted further up the kinetic chain.
Diagnosis
People who overpronate have flat feet or collapsed arches. You can tell whether you overpronate by wetting your feet and standing on a dry, flat surface. If your footprint looks complete, you probably overpronate. Another way to determine whether you have this condition is to simply look at your feet when you stand. If there is no arch on the innermost part of your sole, and it touches the floor, you likely overpronate. The only way to truly know for sure, however, is to be properly diagnosed by a foot and ankle specialist.
Non Surgical Treatment
Overpronation is a condition in which the foot rolls excessively down and inward. The arch may elongate and collapse (or ?fall?) and the heel will lean inward. Overpronation should not be confused with pronation. Pronation is a normal motion of the foot during weight bearing and allows the foot to absorb shock as it contacts the ground.
Surgical Treatment
Depending on the severity of your condition, your surgeon may recommend one or more treatment options. Ultimately, however, it's YOUR decision as to which makes the most sense to you. There are many resources available online and elsewhere for you to research the various options and make an informed decision.
Over-pronation, or flat feet, is a common biomechanical problem that occurs in the walking process when a person?s arch collapses upon weight bearing. This motion can cause extreme stress or inflammation on the plantar fascia, possibly causing severe discomfort and leading to other foot problems.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding stress to other parts of the foot. As a result, over-pronation, often leads to Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
Overpronation can be a contributing factor in other lower extremity disorders, such as foot pain, plantar fasciitis, ankle injuries, medial tibial stress syndrome (shin splints), periostitis, stress fractures and myofascial trigger points. Overpronation increases the degree of internal tibial rotation, thereby contributing to various knee disorders such as meniscal injury or ligament sprains. The effects of the postural deviation are exaggerated in athletes due to the increase in foot strikes while running and the greater impact load experienced. When running, three to four times the body weight is experienced with each foot strike.2 If overpronation exists, the shock force is not adequately absorbed by the foot and is transmitted further up the kinetic chain.
Diagnosis
People who overpronate have flat feet or collapsed arches. You can tell whether you overpronate by wetting your feet and standing on a dry, flat surface. If your footprint looks complete, you probably overpronate. Another way to determine whether you have this condition is to simply look at your feet when you stand. If there is no arch on the innermost part of your sole, and it touches the floor, you likely overpronate. The only way to truly know for sure, however, is to be properly diagnosed by a foot and ankle specialist.
Non Surgical Treatment
Overpronation is a condition in which the foot rolls excessively down and inward. The arch may elongate and collapse (or ?fall?) and the heel will lean inward. Overpronation should not be confused with pronation. Pronation is a normal motion of the foot during weight bearing and allows the foot to absorb shock as it contacts the ground.
Surgical Treatment
Depending on the severity of your condition, your surgeon may recommend one or more treatment options. Ultimately, however, it's YOUR decision as to which makes the most sense to you. There are many resources available online and elsewhere for you to research the various options and make an informed decision.
How To Diagnose Calcaneal Apophysitis?
Overview
Sever's Disease is one of the most common causes of heel pain in active adolescents. Hip stability is restored using a non-surgical positioning device. Symptoms of Sever's disease are relieved through a combination of conservative treatment options and preventative measures can be taken to decrease the risk of developing the condition.
Causes
The calcaneal apophysis develops as an independent center of ossification (possibly multiple). It appears in boys aged 9-10 years and fuses by age 17 years, it appears in girls at slightly younger ages. During the rapid growth surrounding puberty, the apophyseal line appears to be weakened further because of increased fragile calcified cartilage. Microfractures are believed to occur because of shear stress leading to the normal progression of fracture healing. This theory explains the clinical picture and the radiographic appearance of resorption, fragmentation, and increased sclerosis leading to eventual union. The radiographs showing fragmentation of the apophysis are not diagnostic, because multiple centers of ossification may exist in the normal apophysis, as noted. However, the degree of involvement in children displaying the clinical symptoms of Sever disease appears to be more pronounced. In a study of 56 male students from a soccer academy, of whom 28 had Sever disease and 28 were healthy control subjects, findings suggested that higher heel plantar pressures under dynamic and static conditions were associated with Sever disease, though it was not established whether the elevated pressures predisposed to or resulted from the disease. Gastrocnemius ankle equinus also appeared to be a predisposing factor.
Symptoms
Symptoms of Sever?s disease, mostly pain at the back of heel, usually occur during and after sporting activity, and usually disappear with rest. In some cases, children may find it difficult to place pressure on their heels, and begin walking on their toes to gain relief. For some children, the heel pain will persist until the next morning, causing some stiffness or hobbling on first arising. Some children may experience mild swelling at the back of the heel.
Diagnosis
Physical examination varies depending on the severity and length of involvement. Bilateral involvement is present in approximately 60% of cases. Most patients experience pain with deep palpation at the Achilles insertion and pain when performing active toe raises. Forced dorsiflexion of the ankle also proves uncomfortable and is relieved with passive equinus positioning. Swelling may be present but usually is mild. In long-standing cases, the child may have calcaneal enlargement.
Non Surgical Treatment
Treatment of Severs disease usually involves a combination of an accurate analysis of your child?s gait, muscles, tendons, ligaments and joints is a crucial first step. Specific stretching and strengthening exercises often make up part of the treatment. Anti-inflammatory measures such as ice baths after exercise can be helpful in the short term. Footwear review, assessment and advice is important. Orthotic devices are often needed to firstly control any abnormal traction or tension on the heel growth plate and, secondly, too unload the ground reaction forces on the heel bone. Podiatry Care has podiatrists with specific paediatric training enabling them to utilise treatment options to relieve heel pain in children very quickly. If your child is struggling to play sport, see a Podiatry Care podiatrist near you. In severe cases modification to activity levels may be required. Treatment of Severs disease does NOT require surgery. This foot condition responds very well to conservative treatment.
Prevention
It is important to undertake correct warm ups and warm downs before and after exercise. This should include a stretching routine. It may be necessary to undertake additional stretching outside of sport, especially during stages of growth. Only playing one sport should be avoided. You should not allow your child to play through pain.
Sever's Disease is one of the most common causes of heel pain in active adolescents. Hip stability is restored using a non-surgical positioning device. Symptoms of Sever's disease are relieved through a combination of conservative treatment options and preventative measures can be taken to decrease the risk of developing the condition.
Causes
The calcaneal apophysis develops as an independent center of ossification (possibly multiple). It appears in boys aged 9-10 years and fuses by age 17 years, it appears in girls at slightly younger ages. During the rapid growth surrounding puberty, the apophyseal line appears to be weakened further because of increased fragile calcified cartilage. Microfractures are believed to occur because of shear stress leading to the normal progression of fracture healing. This theory explains the clinical picture and the radiographic appearance of resorption, fragmentation, and increased sclerosis leading to eventual union. The radiographs showing fragmentation of the apophysis are not diagnostic, because multiple centers of ossification may exist in the normal apophysis, as noted. However, the degree of involvement in children displaying the clinical symptoms of Sever disease appears to be more pronounced. In a study of 56 male students from a soccer academy, of whom 28 had Sever disease and 28 were healthy control subjects, findings suggested that higher heel plantar pressures under dynamic and static conditions were associated with Sever disease, though it was not established whether the elevated pressures predisposed to or resulted from the disease. Gastrocnemius ankle equinus also appeared to be a predisposing factor.
Symptoms
Symptoms of Sever?s disease, mostly pain at the back of heel, usually occur during and after sporting activity, and usually disappear with rest. In some cases, children may find it difficult to place pressure on their heels, and begin walking on their toes to gain relief. For some children, the heel pain will persist until the next morning, causing some stiffness or hobbling on first arising. Some children may experience mild swelling at the back of the heel.
Diagnosis
Physical examination varies depending on the severity and length of involvement. Bilateral involvement is present in approximately 60% of cases. Most patients experience pain with deep palpation at the Achilles insertion and pain when performing active toe raises. Forced dorsiflexion of the ankle also proves uncomfortable and is relieved with passive equinus positioning. Swelling may be present but usually is mild. In long-standing cases, the child may have calcaneal enlargement.
Non Surgical Treatment
Treatment of Severs disease usually involves a combination of an accurate analysis of your child?s gait, muscles, tendons, ligaments and joints is a crucial first step. Specific stretching and strengthening exercises often make up part of the treatment. Anti-inflammatory measures such as ice baths after exercise can be helpful in the short term. Footwear review, assessment and advice is important. Orthotic devices are often needed to firstly control any abnormal traction or tension on the heel growth plate and, secondly, too unload the ground reaction forces on the heel bone. Podiatry Care has podiatrists with specific paediatric training enabling them to utilise treatment options to relieve heel pain in children very quickly. If your child is struggling to play sport, see a Podiatry Care podiatrist near you. In severe cases modification to activity levels may be required. Treatment of Severs disease does NOT require surgery. This foot condition responds very well to conservative treatment.
Prevention
It is important to undertake correct warm ups and warm downs before and after exercise. This should include a stretching routine. It may be necessary to undertake additional stretching outside of sport, especially during stages of growth. Only playing one sport should be avoided. You should not allow your child to play through pain.
Tibial Posterior Tendon Dysfunction Stages
Overview
The majority of people will experience a flattening of the arch of the feet as we age. This is a natural part of the aging process for most, as the years of abuse we put on our feet causes weakening of the soft tissue structures that support the arch of the foot and gravity dictates that the feet tend to flatten out. When flattening of one of the feet occurs rapidly over a relatively short period of time this may signal a more serious problem. 
Causes
Flat footedness, most people who develop the condition already have flat feet. With overuse or continuous loading, a change occurs where the arch begins to flatten more than before, with pain and swelling developing on the inside of the ankle. Inadequate support from footwear may occasionally be a contributing factor. Trauma or injury, occasionally this condition may be due to fracture, sprain or direct blow to the tendon. Age, the risk of developing Posterior Tibial Tendon Dysfunction increases with age and research has suggested that middle aged women are more commonly affected. Other possible contributing factors - being overweight and inflammatory arthritis.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
Diagnostic testing is often used to diagnose the condition and help determine the stage of the disease. The most common test done in the office setting are weightbearing X-rays of the foot and ankle. These assess joint alignment and osteoarthritis. If tendon tearing or rupture is suspected, the gold standard test would be MRI. The MRI is used to check the tendon, surrounding ligament structures and the midfoot and hindfoot joints. An MRI is essential if surgery is being considered.
Non surgical Treatment
A patient who has acute tenosynovitis has pain and swelling along the medial aspect of the ankle. The patient is able to perform a single-limb heel-rise test but has pain when doing so. Inversion of the foot against resistance is painful but still strong. The patient should be managed with rest, the administration of appropriate anti-inflammatory medication, and immobilization. The injection of corticosteroids is not recommended. Immobilization with either a rigid below-the-knee cast or a removable cast or boot may be used to prevent overuse and subsequent rupture of the tendon. A removable stirrup-brace is not initially sufficient as it does not limit motion in the sagittal plane, a component of the pathological process. The patient should be permitted to walk while wearing the cast or boot during the six to eight-week period of immobilization. At the end of that time, a decision must be made regarding the need for additional treatment. If there has been marked improvement, the patient may begin wearing a stiff-soled shoe with a medial heel-and-sole wedge to invert the hindfoot. If there has been only mild or moderate improvement, a longer period in the cast or boot may be tried. 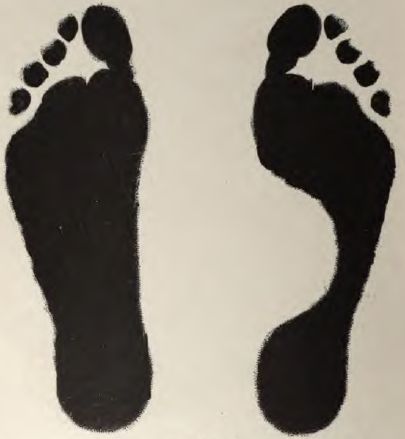
Surgical Treatment
In cases where cast immobilization, orthoses and shoe therapy have failed, surgery is the next alternative. The goal of surgery and non-surgical treatment is to eliminate pain, stop progression of the deformity and improve mobility of the patient. Opinions vary as to the best surgical treatment for adult acquired flatfoot. Procedures commonly used to correct the condition include tendon debridement, tendon transfers, osteotomies (cutting and repositioning of bone) and joint fusions. (See surgical correction of adult acquired flatfoot). Patients with adult acquired flatfoot are advised to discuss thoroughly the benefits vs. risks of all surgical options. Most procedures have long-term recovery mandating that the correct procedure be utilized to give the best long-term benefit. Most flatfoot surgical procedures require six to twelve weeks of cast immobilization. Joint fusion procedures require eight weeks of non-weightbearing on the operated foot - meaning you will be on crutches for two months. The bottom line is, Make sure all of your non-surgical options have been covered before considering surgery. Your primary goals with any treatment are to eliminate pain and improve mobility. In many cases, with the properly designed foot orthosis or ankle brace, these goals can be achieved without surgical intervention.